Carter Bakkum, Senior Consultant, Data & Analytics
Carter is a Senior Consultant of Data & Analytics who works to turn complex, messy data into actionable intelligence. Carter studied economics and statistics at the University of Virginia before joining an economic consulting firm, where he supported expert testifying economic witnesses on behalf of fortune 500 healthcare companies. After the significant changes in the importance of data analytics during the pandemic, Carter joined the Trella team to dive deeper into the numbers to uncover the stories that drive our experience.![]()
Blog
Bite-Sized Trends: Post-Acute Utilization and Pathways for Patients with Sepsis and OAF Diagnoses
By Carter Bakkum | January 13, 2022
As we’ve discussed in earlier blogs, patient care pathways give us a clear view of the route that a patient follows from a given starting point – for our purposes, from the point of discharge from a stay in an acute setting. When we study aggregate patient pathways, we can estimate utilization of certain services and identify patient populations that may be underutilizing specific care settings.
With the rise of value-based care, it’s more important than ever for post-acute care businesses to understand trends and typical behaviors in patient pathways after an inpatient stay. Getting a better understanding of utilization (and underutilization) trends for the patient populations that you serve most will help you make data-informed decisions to avoid financial penalties, increase reimbursements, and growyour business’ market share.
In our ongoing series investigating opportunities for post-acute care agencies, we’ve thus far explored patient pathways for all/high-acuity patients and cardiac/respiratory patients. In this installment, we’ll focus on sepsis patients and inpatient discharges with other abnormal findings (OAF).
Methodology
Using access to 100% of Medicare Part A and B claims data, Trella has followed the care pathway after nearly 677,000 sepsis inpatient discharges and 578,000 inpatient discharges with OAF to understand where Medicare beneficiaries are receiving care after an inpatient stay. Sepsis and OAF patients are determined based on the International Classification of Diseases (ICD-10) codes and aggregated based on similar diagnoses that align with an organ system or related medical specialty. You can find more information on Trella’s approach to diagnostic groupings here.
Tracking patient pathways for sepsis patients
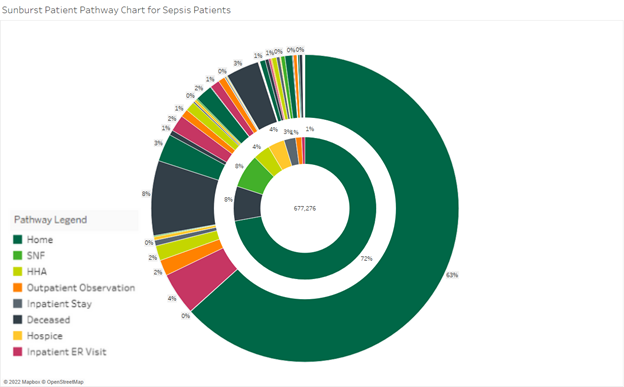
Below is a sunburst chart illustrating the patient pathways for Medicare fee-for-service (FFS) beneficiaries with a primary diagnosis of sepsis discharged from an inpatient stay at a facility with more than 100 discharges between Q3 2020 and Q2 2021. The middle of the chart illustrates the total number of discharges, with each color indicating the first place of care after an inpatient stay. The second layer illustrates the second place of care, dependent on the initial layer.
Some patient pathways are unknown, due to suppression requirements from CMS. We’ve excluded those patients from this analysis, which could bias the results toward larger hospital systems. With that said, this chart illustrates some interesting utilization trends. For example, 8% of total inpatient discharges entered SNF care within two days of inpatient discharge, and only 2% of total inpatient discharges entered a SNF care setting followed by an inpatient ER setting. Further, out of the 488,000 sepsis patients discharged home for at least two days, 9.3% (45,585 patients) were readmitted to an outpatient observation center, an inpatient stay, or the emergency room.
These numbers illustrate potential opportunities for post-acute care agencies. Inpatient and outpatient acute care are both extremely costly, and providers participating in risk-sharing payment programs are more aware than ever of the high cost of their readmission rates. Our previous analyses have shown potentially massive cost savings opportunities for hospitals and health systems that discharge cardiac and respiratory patients to the appropriate post-acute care settings. As we explore the numbers associated with sepsis discharges, we see that there may be a similar but smaller opportunity with patients discharged for sepsis.
Essentially, our analysis here illustrates that post-acute care organizations may have a small opportunity to demonstrate their value to physicians that often treat sepsis. However, our findings – here and in previous investigations in this blog series – indicate that post-acute care agencies would likely benefit more from focusing on cardiac and respiratory patients to grow their census.
Tracking patient pathways for OAF patients
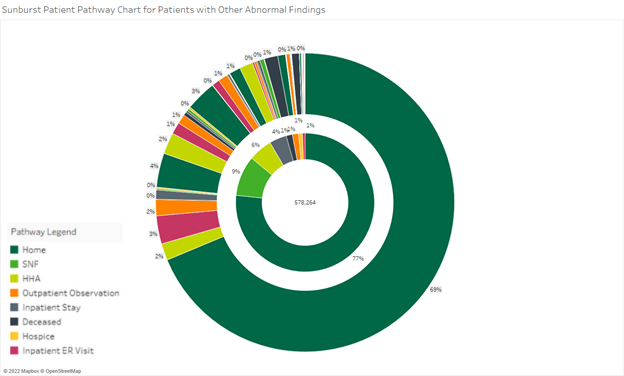
Here we have another sunburst, this time limited to beneficiaries with a diagnosis related to other abnormal findings (OAF). As with our analysis on sepsis patients, unknown patient pathways are excluded. For this analysis, we explored 578,000 inpatient discharges. 77% of OAF patient discharges were discharged home, and 7.5% of these patients were readmitted to an inpatient stay, emergency room, or outpatient observation center. This readmission rate is relatively low, in comparison to other diagnoses. This is to be expected, however, given that the ICD-10 chapter related to abnormal findings captures diagnoses that aren’t fully classified to the same degree of specificity as other ICD-10 chapters. It is highly likely, therefore, that many of these patients were discharged with non-threatening abnormalities that they were able to address with a simple follow-up.
As with our analysis of sepsis patient discharges, our findings here indicated that there may be a small opportunity here for post-acute care agencies to identify patients with some abnormal findings, such as those surrounding the circulatory and respiratory system. However, post-acute care agencies are likely to find much more success in growth by targeting higher-acuity diagnoses.
Next steps: Identify key patient pathways to demonstrate value
Both sepsis and OAF patient populations present small opportunities for post-acute agencies that specialize in these diagnoses. By exploring the available data on key patient populations, post-acute care organizations can identify care gaps and demonstrate areas where they can help acute partners decrease readmits and cost of care while improving patient outcomes. With this data, you can show providers that discharging patients with these diagnoses to your facility could significantly decrease overall cost of care and increase their quality of life.
Trella Health is the leader in market intelligence for the 65+ population, with extensive data sets including Medicare FFS, Medicare Advantage, commercial payers, ACOs, and DCEs. For more insights into how to stand out as a preferred referral partner, schedule a demo today.
About the Author:
