The Hospital Readmission Reduction Program (HRRP) has made 30-day readmissions a key driver of hospital penalties, extending accountability to post-acute providers. As a result, outcome transparency, strong care coordination, and data-driven performance are now essential to reducing risk and maintaining competitive partnerships. This blog explores how post-acute providers can address these challenges and improve readmission performance.
Since its introduction in 2012, the Hospital Readmission Reduction Program (HRRP) has fundamentally reshaped how hospitals and post-acute providers think about care continuity, accountability, and performance. Designed by the Centers for Medicare & Medicaid Services (CMS), the program imposes financial penalties on hospitals when Medicare patients are readmitted within 30 days of discharge for specific conditions. In FY 2013, the program initially tracked readmissions for heart attack, heart failure, and pneumonia. In FY 2015, it expanded to include chronic obstructive pulmonary disease (COPD) and elective hip and knee replacements. The program now targets six specific conditions: heart attack, heart failure, pneumonia, COPD, elective hip and knee replacement, and coronary artery bypass graft (CABG).
While the intent behind HRRP is clear, improving patient outcomes while reducing avoidable costs, the operational reality is far more complex. The program uses the excess readmission ratio (ERR) to assess hospital performance, comparing each hospital’s predicted to expected unplanned readmissions relative to the national average. The cumulative cost of hospital readmissions contributes significantly to overall healthcare expenditures.
The readmission rates for targeted conditions have declined from 21.5% in 2007 to 17.8% in 2015, and readmissions for covered conditions have been reduced more than non-covered conditions. Yet, a significant portion of the responsibility for preventing excess readmissions lies beyond the initial hospital admission and hospitalization period. Departments across the hospital and post-acute continuum must coordinate to manage inpatient care, optimize the hospital stay, and implement strategies to reduce hospital readmissions. By focusing on these areas and monitoring the excess readmission ratio, providers can better align with national benchmarks and improve outcomes.
The Expanding Accountability of Post-Acute Care
Today’s care continuum does not end at discharge. Comprehensive discharge planning begins upon admission, not just on the day of discharge. Patients transitioning to skilled nursing facilities (SNFs), home health agencies, or long-term acute care hospitals (LTACHs) remain, in many ways, an extension of the hospital’s clinical and financial responsibility. If a patient deteriorates due to inadequate follow-up care, poor care coordination, or gaps in clinical oversight, the hospital, not the post-acute provider, bears the financial consequences.
Identifying the index admission and tracking new admissions and unplanned readmissions within 30 days are essential for measuring hospital performance under programs like the Hospital Readmission Reduction Program. Unplanned readmissions, which refer to any new admission that occurs unexpectedly after discharge, are a key metric for assessing quality and determining penalties.
This dynamic has elevated post-acute providers from downstream participants to critical partners in risk management. Hospitals are now compelled to ask difficult questions:
- Which partners consistently prevent avoidable readmissions?
- Where are care gaps most likely to occur?
- How can collaboration be strengthened across settings?
Unfortunately, historically, these questions have been difficult to answer with confidence.
The Visibility Gap
One of the central challenges in managing readmissions is a lack of actionable, transparent data. A systematic review of the literature identifies multiple factors and other factors that influence hospital readmissions, including clinical, demographic, and social determinants. For years, hospitals have relied on limited or lagging indicators when evaluating post-acute performance. Predictive modeling tools can help identify high-risk patients who need intensive post-discharge support. Similarly, many post-acute providers have operated without a clear understanding of how their outcomes compare to competitors or how they are perceived by referral sources.
This “visibility gap” has led to a misalignment in expectations and performance. Hospitals may unknowingly refer patients to underperforming providers, while high-performing organizations struggle to differentiate themselves in a crowded market. Information sharing and efforts to improve communication between hospital staff, primary care providers, and patients are essential to close this gap and reduce avoidable readmissions.
In an environment where even marginal improvements in readmission rates can translate into significant financial impact, operating without data is no longer sustainable.
Readmission Rates as a Competitive Differentiator
As HRRP pressures have intensified, 30-day readmission rates have emerged as one of the most critical metrics in post-acute care. The excess readmission ratio (ERR) is used to compare a hospital’s predicted to expected unplanned readmissions, and hospitals with higher rates face greater financial penalties. Hospital performance is evaluated relative to the national average and compared to other hospitals. These metrics are no longer simply a measure of quality; they are a determinant of market access. Payments, reimbursement, and payment reductions under the Hospital Readmission Reduction Program (HRRP) are directly tied to a hospital’s readmission rates.
Post-acute providers with elevated readmission rates often experience a gradual erosion of referral volume. Hospitals, seeking to protect their margins and quality scores, increasingly narrow their preferred provider networks to include only those organizations that demonstrate consistent, measurable performance.
Conversely, providers with strong outcomes are rewarded with increased referrals, deeper strategic partnerships, and greater influence in care coordination decisions.
This shift represents a broader industry trend: performance transparency is becoming the foundation of partnership.
What Post-Acute Providers Can Do
To succeed in this evolving landscape, post-acute organizations must take a proactive, data-driven approach to managing readmissions. Addressing social determinants of health and partnering with community organizations are essential to reduce hospital readmissions and improve patient outcomes.
1. Invest in Outcomes Intelligence
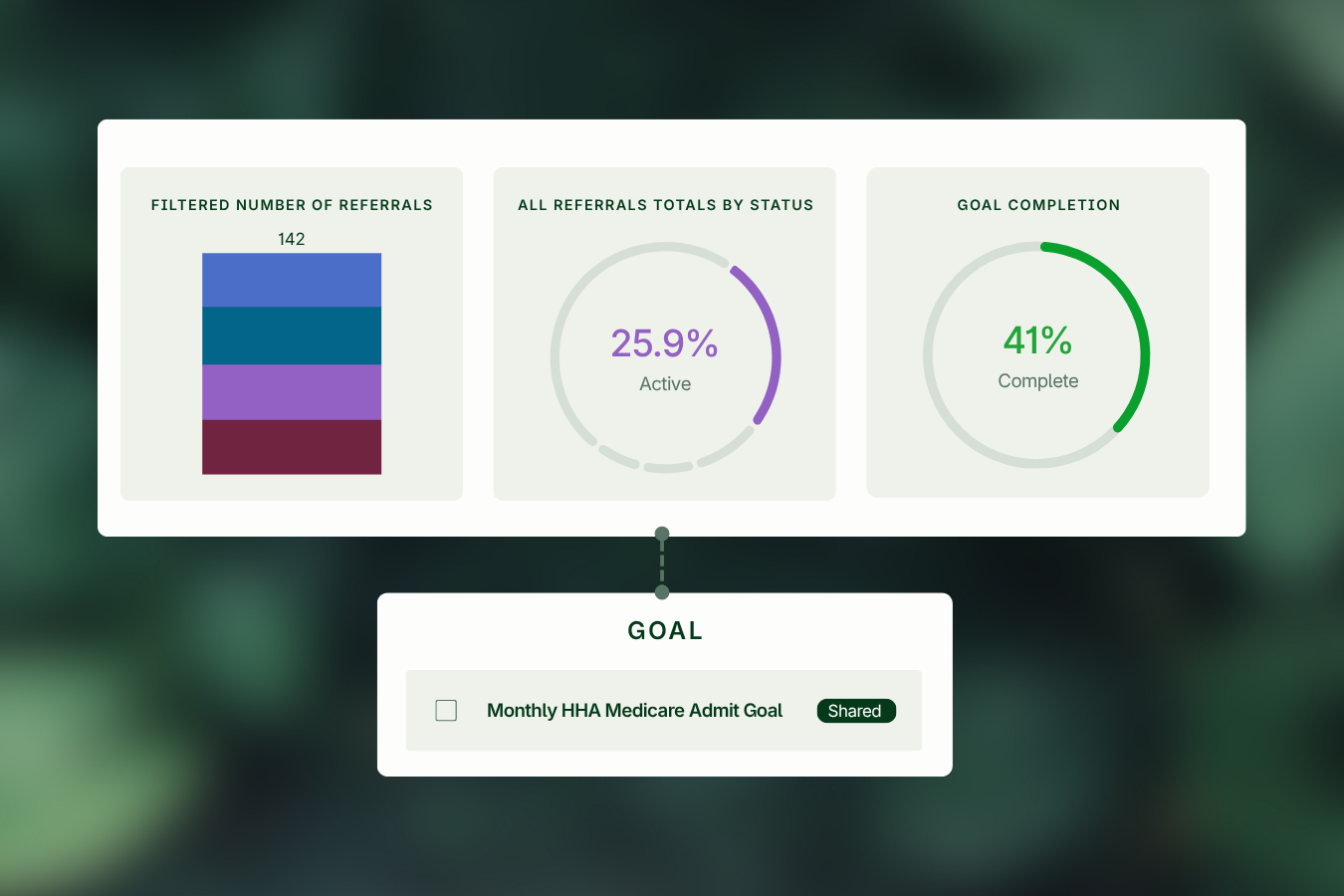
Providers must track readmission rates by diagnosis, referral source, discharge setting, and patient cohort to gain a comprehensive understanding of performance. They should benchmark these outcomes against local and national peers using claims-based datasets to establish context and identify gaps.
Analyzing trends over time is essential for uncovering improvement opportunities and measuring the impact of interventions. Additionally, drilling into episode-level data enables organizations to better understand the underlying drivers of readmissions.
2. Strengthen Care Transitions
Organizations should surface referral source insights to better understand which hospital partners are associated with higher readmission rates. Gaining visibility into discharge patterns helps identify where breakdowns in transitions may occur. By examining these patterns, providers can also uncover gaps in continuity of care across settings and take steps to address them proactively.
3. Identify High-Risk Patients Early
Providers should segment patient populations based on their likelihood of readmission to prioritize interventions more effectively. Identifying patterns in patient characteristics that correlate with poor outcomes allows organizations to focus resources where they will have the greatest impact.
4. Align Clinically and Operationally with Hospital Partners
Organizations should identify top-performing partners as well as opportunities to strengthen alignment across the care continuum. Leveraging data to support conversations around preferred provider status and network optimization enables more strategic and mutually beneficial partnerships.
5. Differentiate Through Transparency
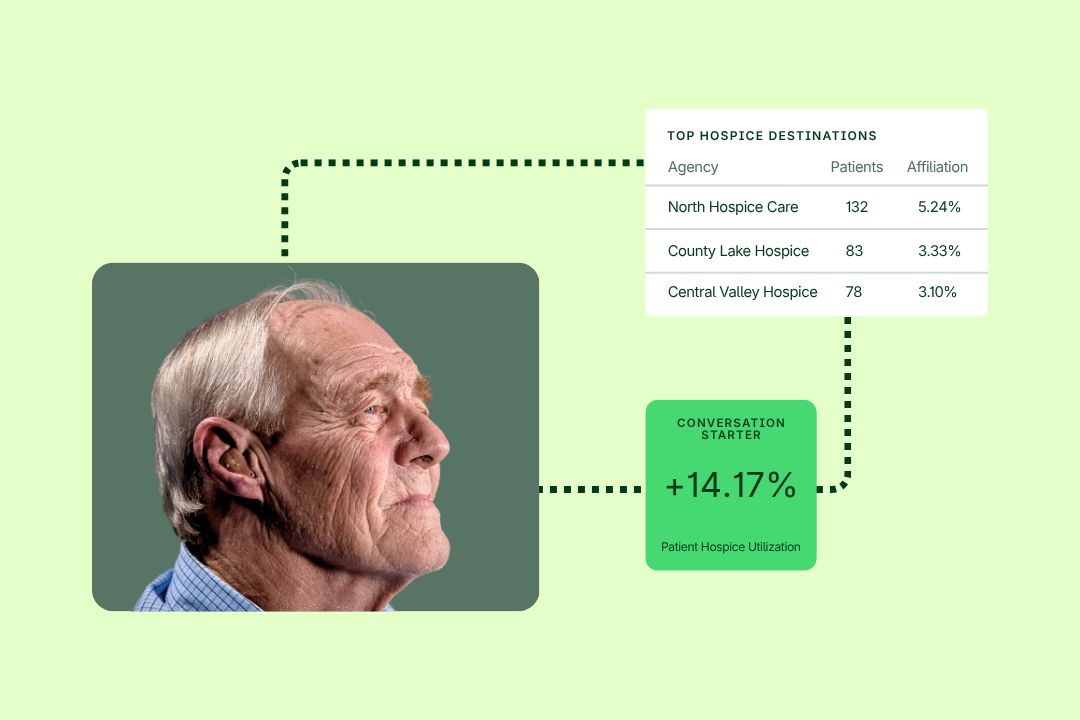
Providers must clearly showcase their readmission rates, patient outcomes, and cost efficiency metrics to referral partners. Delivering consistent, standardized metrics ensures that performance can be easily understood and compared in sales and partnership discussions. Supporting these conversations with data-driven storytelling reinforces organizational value in an increasingly competitive referral landscape.
Turning Insight into Advantage with Trella Health
As the industry moves toward greater accountability and transparency, access to reliable, actionable data has become a strategic imperative. This is where Trella Health distinguishes itself as a preferred solution for post-acute providers and hospitals alike.
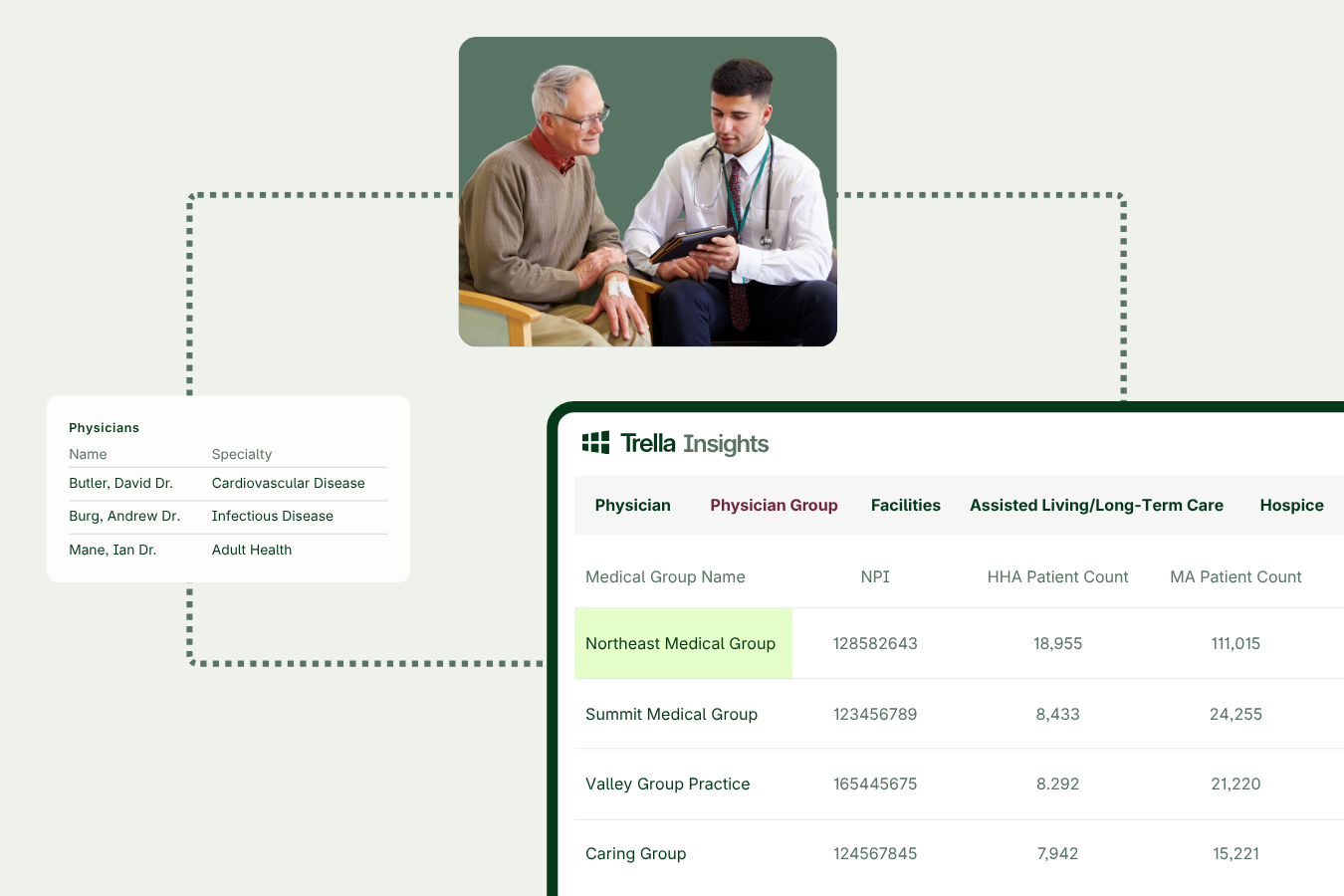
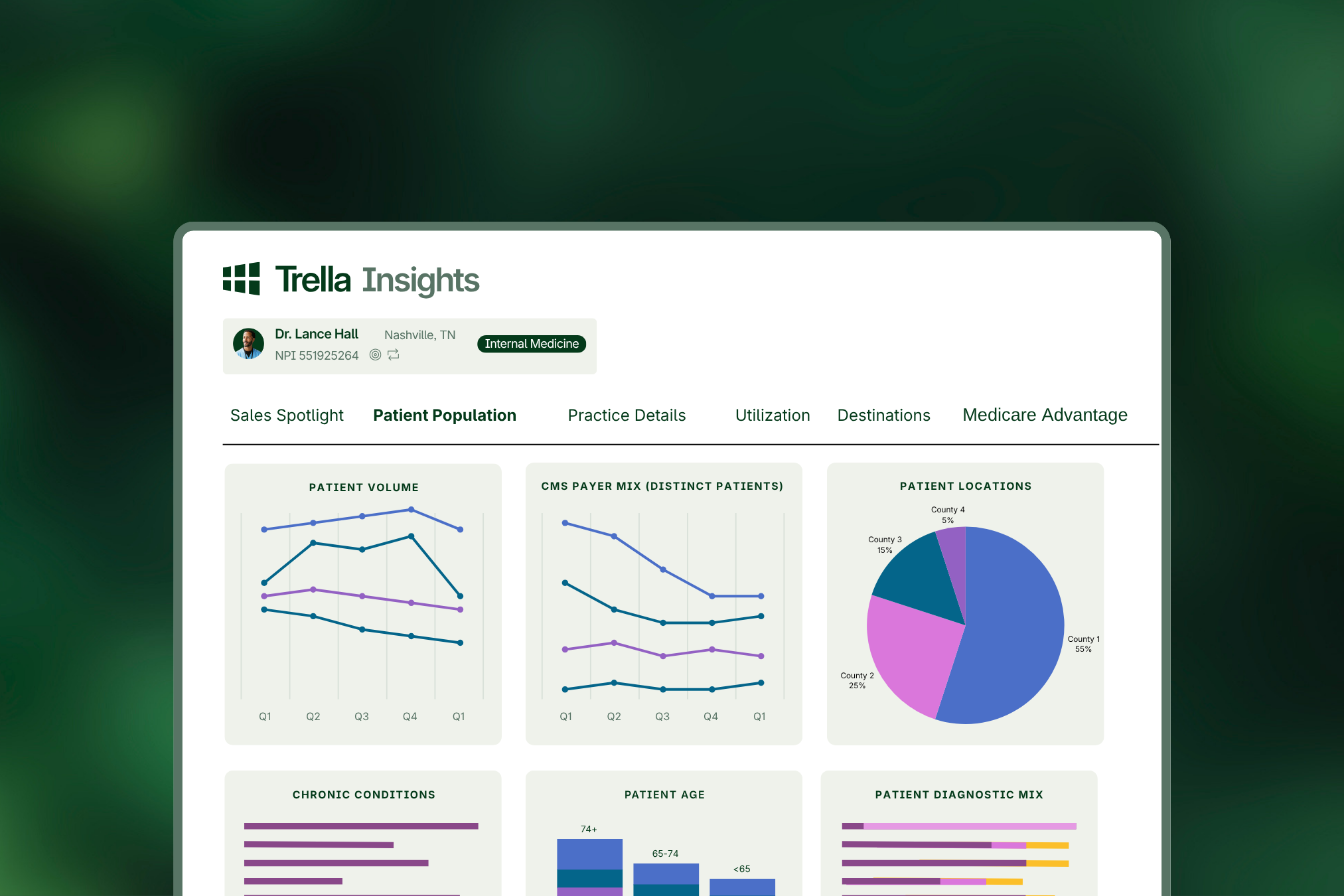
Trella Health equips organizations with comprehensive, market-level insights into referral patterns, patient outcomes, and readmission performance. By illuminating how providers truly perform, not just internally, but relative to competitors, Trella enables more informed, data-driven decision-making across the care continuum.
For post-acute providers, this means the ability to:
- Accurately benchmark readmission rates and identify areas for improvement
- Demonstrate value to hospital partners with credible, third-party data
- Target high-value referral sources aligned with their strengths
For hospitals, it provides the visibility needed to build high-performing post-acute networks that reduce risk and improve patient outcomes.
In an era where readmission performance directly impacts both financial stability and market position, data is no longer optional; it is foundational. Organizations that embrace transparency and leverage advanced analytics will not only navigate HRRP pressures more effectively but also emerge as leaders in a rapidly evolving healthcare landscape.
Connect with a product expert today to learn more.