This article explores how Centers for Medicare & Medicare Services (CMS) Transforming Episode for Accountability Model (TEAM), rising value-based care expectations, and growing accountability around readmissions are reshaping transitional care. It highlights why hospitals must modernize discharge workflows, strengthen post-acute networks, and use data-driven insights to improve outcomes — and how Trella Health and Repisodic provide the tools to support TEAM-ready coordination.
The demands placed on hospitals and health systems have never been higher. CMS growing emphasis on care transitions, the continued spread of value-based care (VBC) models, and rising expectations around readmissions, communication, and patient experience are reshaping how organizations must approach care coordination.
The Transforming Episode Accountability Model (TEAM) accelerates this shift. TEAM elevates the stakes for hospitals, requiring more rigorous post-discharge visibility, tighter alignment with post-acute partners, and greater responsiveness to patient needs across the care continuum. At the same time, healthcare organizations are navigating escalating operational demands, workforce constraints, and increasing pressure to demonstrate measurable improvements. Notably, approximately 20% of Medicare beneficiaries experience readmission within 30 days, highlighting the scale of the issue and the importance of targeted interventions.
To keep pace, hospitals must modernize care transitions; moving beyond manual discharge workflows and fragmented provider relationships toward data-driven coordination supported by digital tools. Reducing hospital readmissions is crucial not only for patient well-being but also for addressing the financial implications faced by healthcare systems, aligning with the broader goals of improved outcomes and cost efficiency.
This blog outlines why the transitional care environment is evolving so quickly and how hospitals can strengthen their strategy through better data, smarter workflows, and innovative partnerships.
The Transitional Care Challenges Hospitals Face Today
Even as transitional care becomes central to performance, many organizations continue to rely on structures and processes that no longer support the expectations of VBC or CMS TEAM. Hospital readmissions are a key metric for quality of care, and high readmission rates can indicate gaps in care transitions and post-discharge support. Common challenges include:
- Fragmented and Manual Discharge Workflows: Static provider lists and repeated phone calls slow down case managers and limit their ability to provide personalized, informed recommendations.
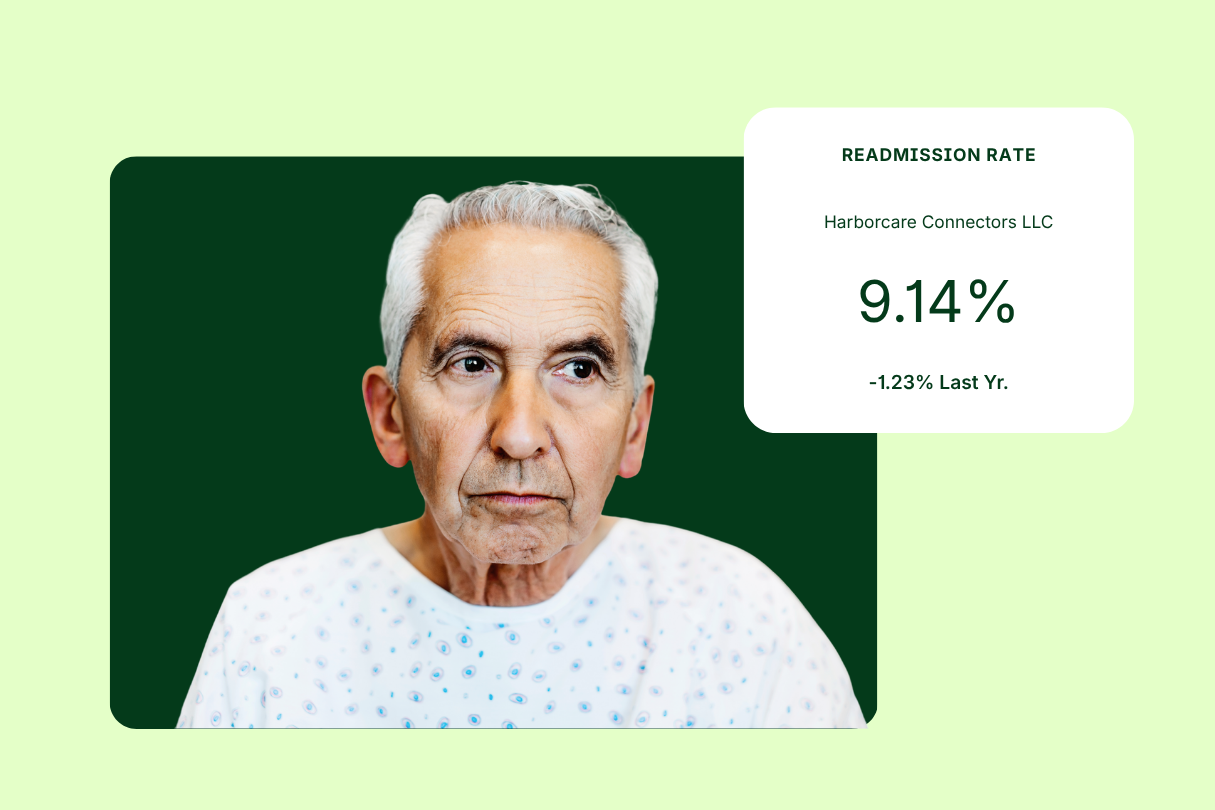
- Escalating Readmission Pressure: As penalties grow and value-based benchmarks tighten, uncoordinated transitions directly impact hospital performance, especially through preventable and unplanned readmissions, which increase the financial impact on hospitals.
- Limited Visibility into Post-Acute Provider Performance: Without data on quality, readmissions, capacity, or episode trends, aligning patient needs with the right post-acute partner becomes guesswork.
- Network Leakage and Referral Variability: Patients frequently leave preferred networks due to inefficient workflows or lack of coordinated referral pathways.
- Increasing Expectations Under CMS TEAM: TEAM emphasizes timely follow-up, patient engagement, data-sharing, and episode accountability; requirements that surpass the capabilities of many existing workflows.
- Staffing Burden and Workflow Inefficiencies: Case managers are stretched thin, spending too much time on administrative tasks and too little on high-value coordination.
These challenges make it increasingly difficult for hospitals to deliver consistent, high-quality transitions at scale.
How CMS TEAM Is Elevating Transitional Care and Hospital Discharge Planning Standards
TEAM is reshaping expectations in ways that directly influence operational priorities. The model pushes hospitals toward:
- More structured and transparent handoffs
- Real-time coordination with post-acute partners
- Detailed episode analytics and root-cause insights
- Routine follow-up and patient engagement
- Higher alignment between patient needs and provider capabilities
TEAM makes clear that transitional care must evolve from reactive discharge processes to proactive, analytics-enabled coordination. The model is designed to incentivize improvements in patient outcomes while sharing financial risk among participants, aligning provider incentives with both quality and cost-saving goals.
Data as the Foundation of Modern Transitional Care
Strong transitional care begins with visibility into patient needs, provider performance, episode trends, leakage drivers, and readmission contributors. Hospitals that lack this intelligence struggle to identify gaps, target performance improvement efforts, or refine their post-acute strategy. Data is essential for tracking hospital readmission rates, analyzing trends, and informing reduction program strategies that aim to decrease unnecessary readmissions and improve patient outcomes.
Data empowers organizations to:
- Match patients to top-performing post-acute partners
- Identify which providers drive avoidable readmissions
- Highlight utilization patterns and care-transition gaps
- Benchmark performance across service lines and populations
- Optimize preferred network structure and accountability
- Support utilization projects focused on reducing hospital readmission rates through targeted interventions
The transition to TEAM and VBC requires hospitals to move beyond anecdotal decision-making. Consistent, comprehensive data becomes the foundation for reliable, repeatable, and scalable improvement.
From Insight to Action: Moving Toward TEAM-Ready Coordination
Understanding the importance of data is only the first step. Hospitals must be able to operationalize insights within everyday workflows, supporting case managers, informing discharge decisions, and aligning network partners. Enhancing communication between care teams, patients, and post-acute providers is crucial for improving information transfer, reducing errors, and ensuring all parties are aligned during care transitions. Achieving TEAM readiness requires tools that connect analytics with action.
This is where solutions such as Trella Health and Repisodic become essential: they bridge the gap between visibility and execution. TEAM quality measures focus on care coordination, patient safety, and patient-reported outcomes.
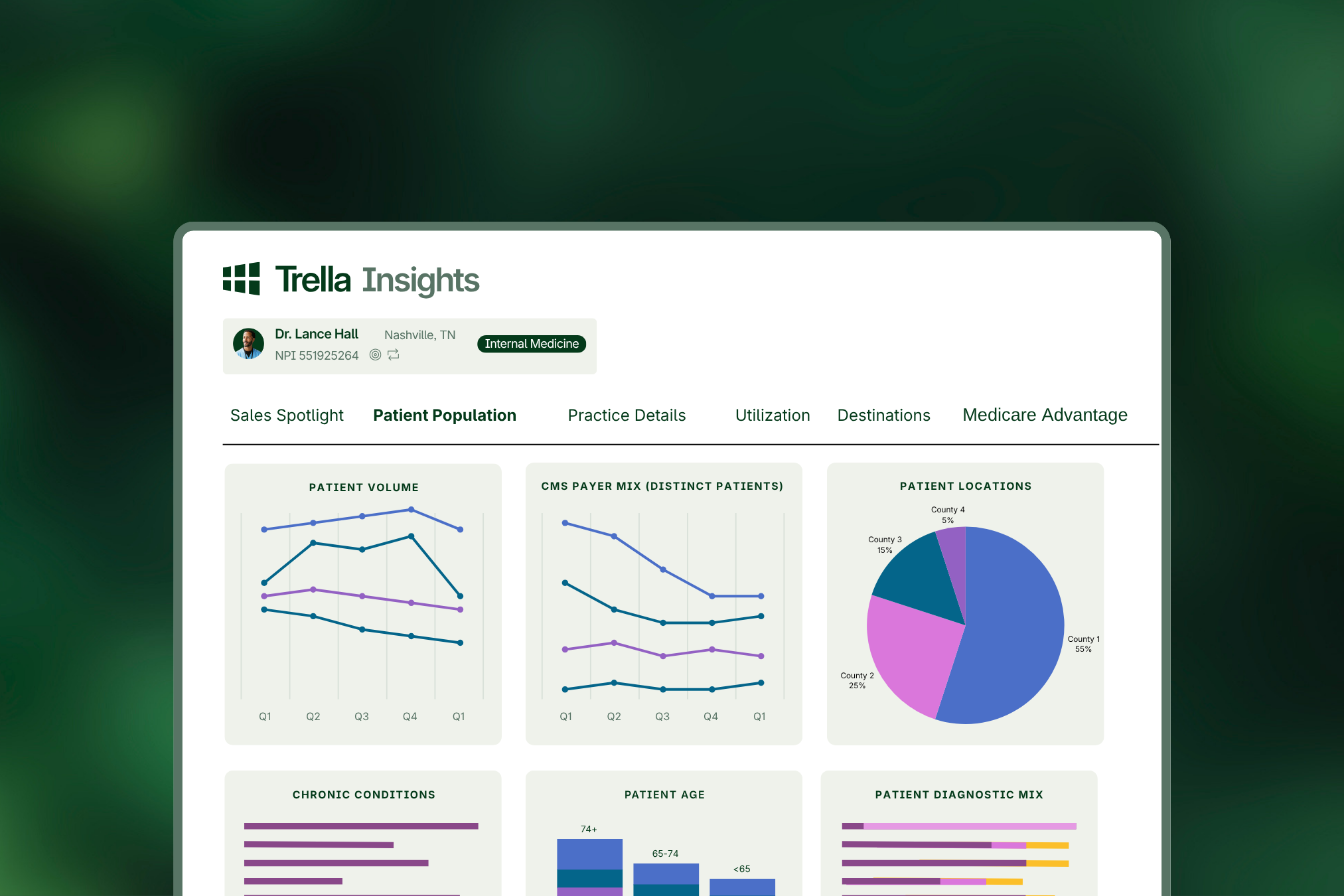
Trella Health: Illuminating Performance, Partners, and Opportunities
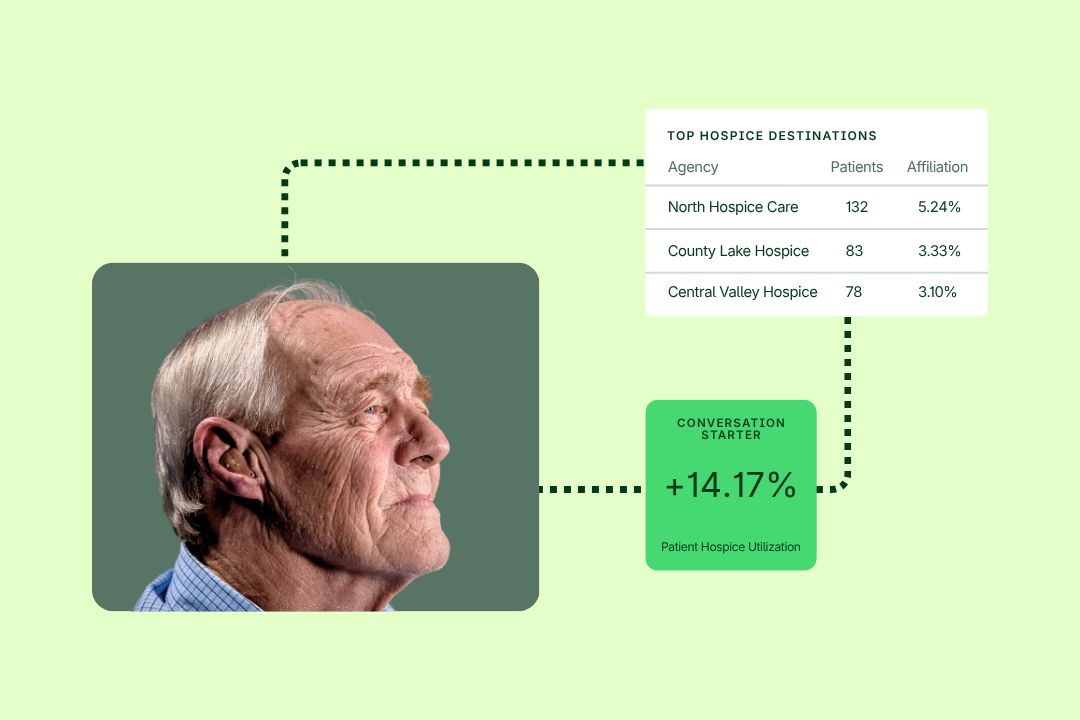
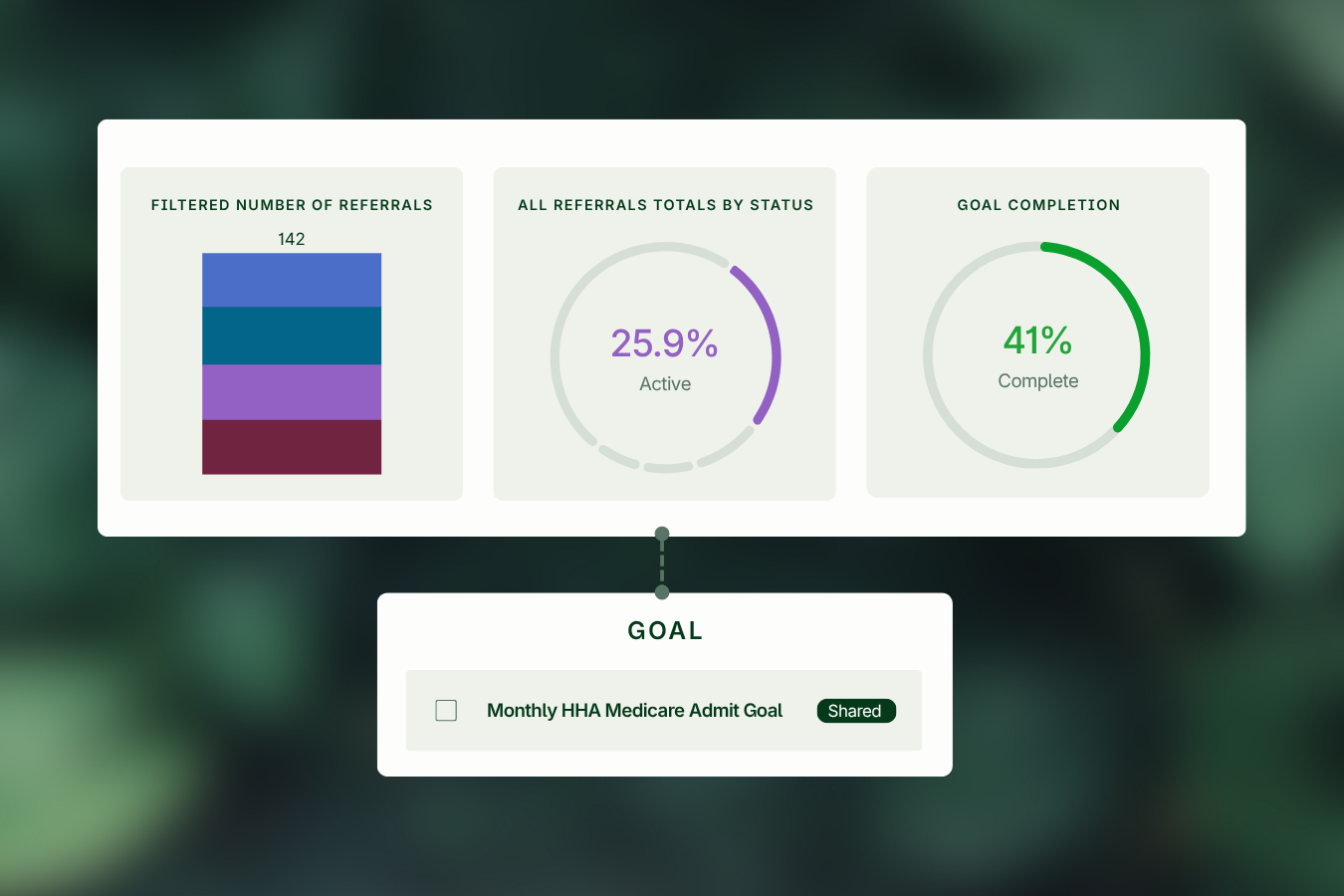
Trella Health’s TEAM Metrics gives hospitals the insight needed to understand episode-level performance and post-acute alignment. These metrics provide:
- Readmission contributors and episode trend analysis
- Performance benchmarking for SNFs, HHAs, and other PAC providers
- Leakage insights and referral alignment metrics
- Identification of gaps in coordination, quality, and outcomes
Through these metrics, hospitals gain the clarity required to build stronger networks, refine strategy, and improve their readiness for TEAM accountability.
Want to explore TEAM Metrics in action? Watch this on-demand webinar to learn more post-acute partners can better navigate the TEAM landscape.
Repisodic: Digitizing and Streamlining the Discharge Workflow
Repisodic modernizes the discharge process with a digital platform designed to reduce friction and support patient-centered choice. The platform delivers:
- Real-time provider data on quality, capacity, and services
- Dynamic, guided referral workflows for case managers
- Digital patient engagement tools to support informed decisions
- Automated workflows that reduce administrative burden and delays
This digital infrastructure strengthens handoffs, increases efficiency, and ensures patients transition smoothly into the right post-acute setting.
A Combined Approach for Transitional Care Excellence
 Individually, analytics and digital workflows improve transitional care. Together, they create a comprehensive foundation for TEAM performance.
Individually, analytics and digital workflows improve transitional care. Together, they create a comprehensive foundation for TEAM performance.
By integrating Trella Health’s TEAM Metrics with Repisodic’s digital discharge capabilities, hospitals can:
- Reduce readmissions
- Improve referral efficiency
- Strengthen preferred network alignment
- Enhance patient experience and engagement
- Streamline case manager workflow
- Elevate VBC performance across service lines
Hospitals that embrace this unified approach position themselves at the forefront of modern, data-driven transitional care.
Ready to align discharge workflows and insights for advanced patient-centered outcomes? Watch this on-demand webinar to learn more.
Building a TEAM-Ready Future
CMS TEAM signals a future where hospitals are held accountable not only for discharge decisions but for the outcomes that follow. The organizations that thrive will be those that integrate high-quality data, modern technology, and strategic collaboration into every step of the transition process.
With Trella Health and Repisodic, hospitals have the intelligence and tools needed to meet these expectations; transforming care transitions into a strategic advantage rather than an operational challenge.
By adopting a more connected, data-driven approach today, healthcare leaders can strengthen their networks, improve performance, and prepare confidently for the next era of transitional care.